English
English
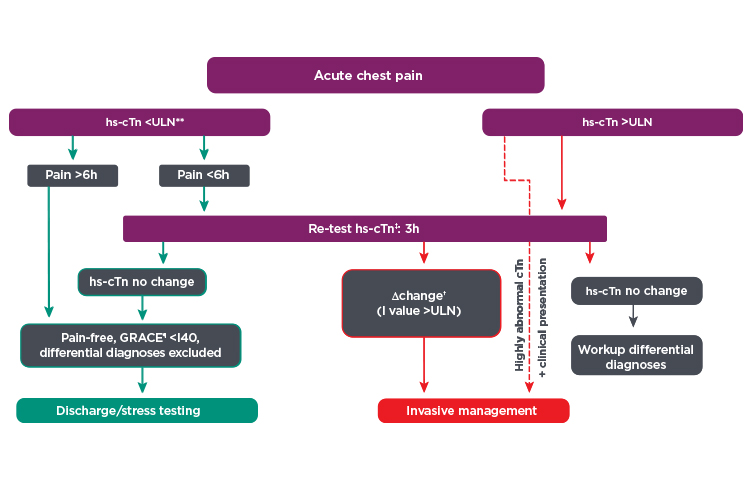
High sensitivity troponin tests detect circulating troponin at lower levels and provide improved diagnostic clarity. These tests can accelerate decision making and improve patient care. To qualify as true high sensitivity troponin assays, these tests should:
- Meet IFCC guidelines for high sensitivity troponin testing1
- Detect cTn above the Limit of Detection in >50% of healthy populations
- Achieve 10% CV below the 99th percentile URL
- Support current cardiac guidelines for patient management
- Provide sex-specific thresholds that may generate more accurate diagnoses for women